

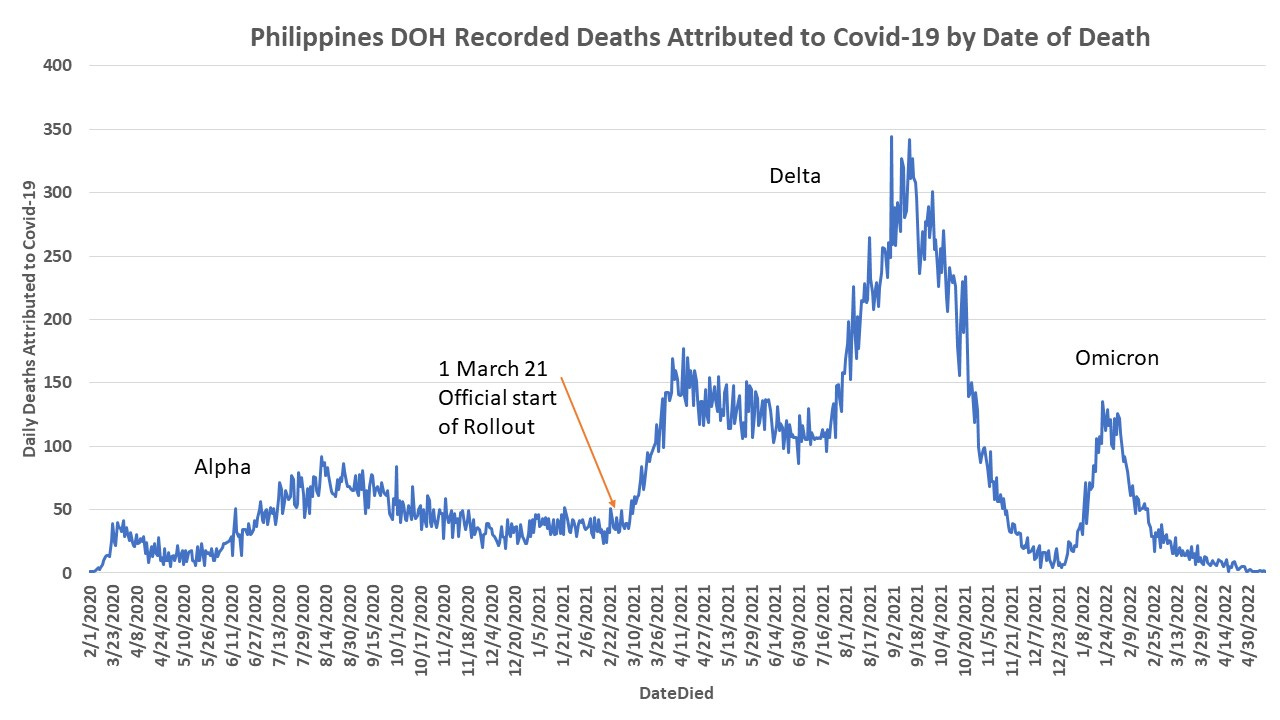
Analysis of Philippines DOH Covid-19 Tracking Data at 11 June 2022: Total Deaths, Age and Gender Distribution by year, and Positive Specimen Collection Relative to Date of Death.
Pattern of Covid-19 Deaths has shifted to younger populations over time. Most reported deaths occurred the same day as test specimen collection or within 1-14 days post test. Some data discrepancies.

An analyses of available covid-19 attributed death data from Philippines DOH shows 60,164 total deaths, of which 55% are men and 45% are women. The latest recorded death in this data file was 7th of June 2022.
I analyzed the data to see the number of days between the sample collection and death. If date of sample collection was not avialable I referred to the date of result release, or if that was not available by the data of report confirmed.
93% of deaths have both a “DateSpecimen” and a “DateDied”. 539 reports (0.9%) have a “DateResultRelease” and a “DateDied”, and 3,598 reports (5.98%) have only a “DateRepConf” and a “DateDied”.
Most deaths were recorded to have occurred between -1 to +14 days following a positive test. While 19.3% of people died same day they were tested, another 3% were tested the 1st or 2nd day after they had died. In the Philippines during the pandemic, no person was admitted to any hospital or their body allowed to be handed after death, without a covid-19 test. All positive results were compulsorily cremated. In some cases this was done by the local government, sparing the bereaved family that cost.
Thus, officially, all deaths were tested for covid-19 and a status of positive or negative assigned. Covid-19 may have been an inadvertent finding for these people who died the same day as being tested or who were tested after death, however, it was used to calculate death numbers, and flame fear and demand for the vaccines.
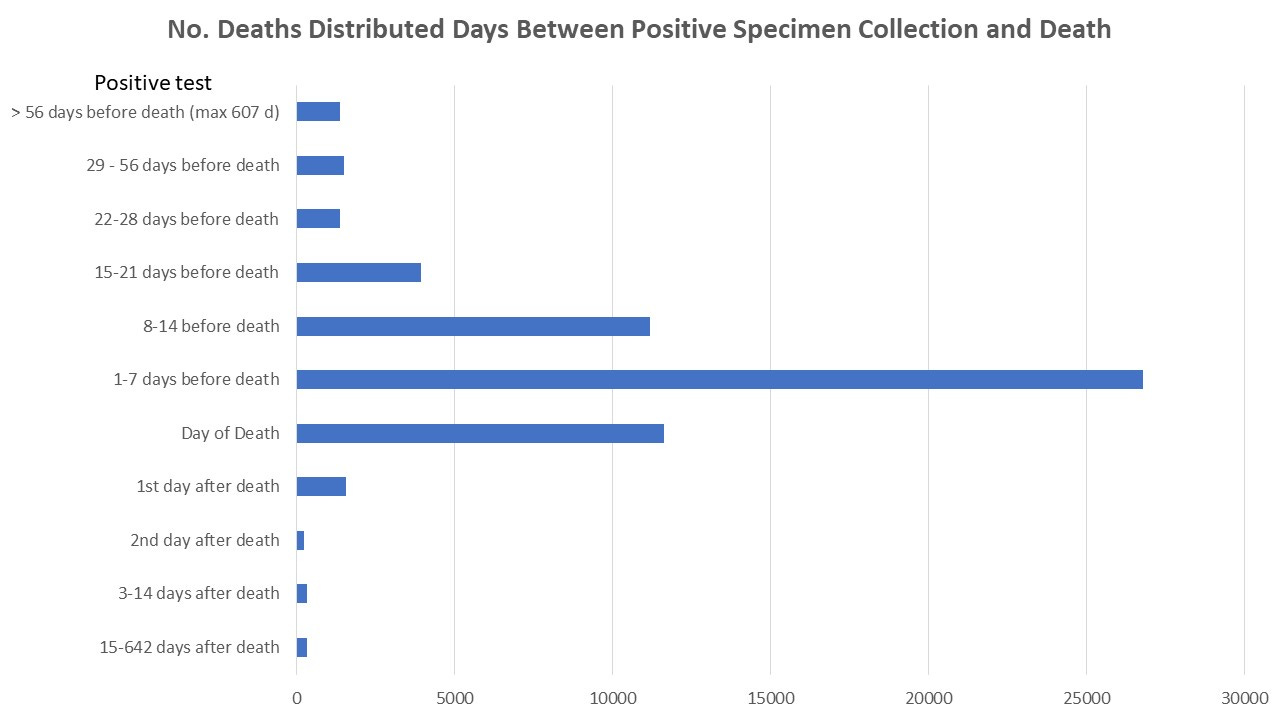
The negative extreme outliers (test is reported as having been done weeks to months after the person had already died) could perhaps represent data entry error? The positive extreme outliers could also be data error, could be used to obscure other death causes (AEFI?), or could be simply using any past positive test to bump case and death numbers.
Breakdown of deaths by age and gender changed in each year of the pandemic. Though absolute deaths are far less in 2022 so far, the distribution of deaths has moved notably into younger age groups.
In the first year of the pandemic male deaths made up the largest % at 60%. Females % deaths rose in 2021 to 46% (could that be to do with female care givers having been prioritized for vaccination, and there were stories of entire hospital departments coming down with covid-19, with deaths, immediately following vaccination in 2021), though their % has come down again slightly in 2022 to 44%?
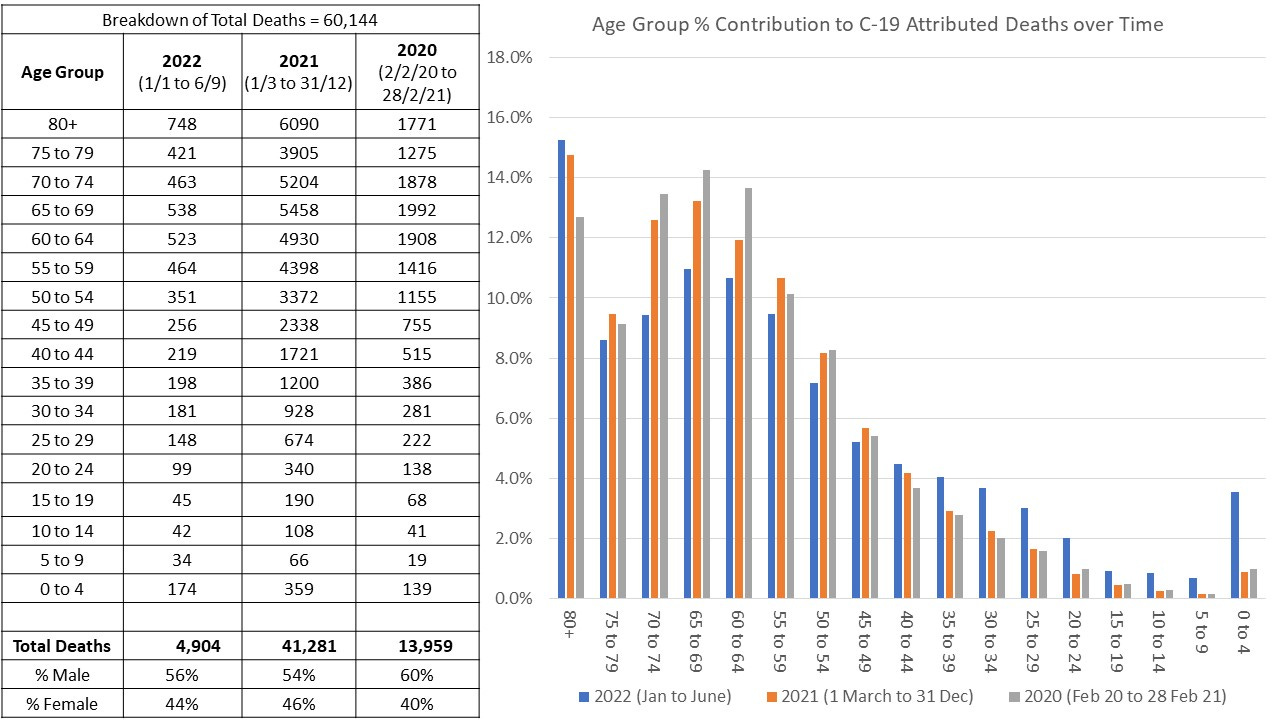
Vaccination, as a key evolution pressure on the C-19 virus, appears to have pushed covid-19 towards age-groups that were not previously susceptible. This is curious, as Omicron, the main variant in 2022, is recognized to be less pathogenic though more infectious. There could be other factors changing susceptibility, such as immune system modification, affecting host ability to deal with the illness. The 0-4 age group has not been vaccinated, however, their susceptibility appears to have changed negatively. The very elderly also fared worse in 2022.
So much for protection of the vulnerable!
I truly appreciate your presentation of our COVID statistics. Is it possible to show the deaths per 100,000 aside from just total deaths? Also, percent contribution of each age group to total deaths?
Also, I remember the PSA undersecretary who spoke in a seminar sponsored by the UP Population Institute, claiming that there are more COVID deaths than previously thought because they adjusted for the deaths of COVID positives and presumed positives, whether or not the deaths were due to COVID, instead of simply relying on the death certificate entry naming COVID and complications as the direct cause of death. A "presumed COVID" on the death certificate would be counted as a COVID death. And anyone who comes into the ER with a fever was automatically presumed COVID during the days when a PCR diagnosis took days if not weeks to receive.
This is on top of the already padded death statistics specially during the time that COVID diagnosis and death was inventivised in hospitals in the early months of the pandemic. Such that even vehicular accidents were recorded as COVID deaths.
This might explain the country's abnormally high case fatality ratio for COVID.